In a world where the majority — 60% to 80% — of people don’t follow their prescribed treatment, pharma manufacturers continue to struggle to address the health consequences and financial burden of non-
In a world where the majority — 60% to 80% — of people don’t follow their prescribed treatment, pharma manufacturers continue to struggle to address the health consequences and financial burden of non-
adherence. Education, reminder tactics, points for prizes and gaming techniques; there are many options positioned as solutions. Yet, not all adherence solutions are created equal.
The industry is now preaching behavior change as the “secret sauce" to solving the adherence puzzle. Of course we want nonadherent people to change their behaviors around their prescribed treatment, including medicines and/or lifestyle habits. But how can we successfully achieve that change, for the long-term?
Telling someone to follow prescribed treatment or reminding them to do so isn’t always a successful strategy for long-term adherence. To be successful, behavior change models need to look at the reasons behind the behavior.
Understanding Why
The discipline of health psychology, a well-known academic discipline recently being applied to commercial business in the United States, provides us with proven models to understand why people are nonadherent. The logic is fairly simple — you need to understand what beliefs are driving the behavior you want to change, or the “why," before you can successfully change that behavior long-term.
The application of health psychology to treatment adherence is based on three principles:
1. A person’s nonadherence to medication or suggested lifestyle changes is a behavior
2. Behaviors are influenced by a person’s individual belief system (thoughts, perceptions and other factors)
3. Improving adherence requires a person to change their unhelpful beliefs
As simple as the logic is, the process requires skilled specialists to implement successfully.
Behavior Change Tools
 No doubt you’ve heard about motivational interviewing. It’s become the Kleenex of behavior change. In reality, this is just one of dozens of behavior change technique tools being used to change patient beliefs that drive behavior.
No doubt you’ve heard about motivational interviewing. It’s become the Kleenex of behavior change. In reality, this is just one of dozens of behavior change technique tools being used to change patient beliefs that drive behavior.
For an intervention to be truly effective, there first needs to be research to understand the beliefs behind the behaviors. That understanding will help identify which types of behavior change techniques should be leveraged within a specific program. It may be motivational interviewing, but could also be tools like goal setting or action planning.
Research drives a more personalized approach to behavior change.
Personalization vs. Segmentation
Pharma often segments people based on where they may be in the illness or treatment cycle, demographics like age, socio-economic status, or other factors like personality or motivation. These can be helpful to know and build upon, but health psychologists are trained to view illness and adherence through a more personalized lens. They develop research to understand why people with the same condition on the same medication and similar socio-demographics choose to adhere to their prescribed treatment to different degrees, or not at all. Even within a segment (e.g., early adopter), people’s beliefs — and therefore their behaviors — are unique to them.
Health psychology models are used to understand why people behave in such different ways in managing their illness, whether it’s in the context of taking medicines according to a prescribed schedule, being alert to side effects or changing their unhealthy lifestyle habits. By applying academic rigor in the research stage, we can better understand the beliefs and behaviors exhibited by our audience, and work to design interventions to target the unhelpful beliefs that drive unhelpful behaviors to move the needle in adherence metrics.
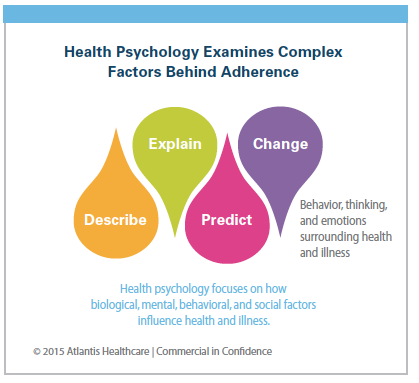
Health Psychology Examines Complex Factors Behind Adherence Factors that Influence Beliefs
 The factors that drive behavior are multi-factorial and complex. One health psychology theory divides behavioral factors into three groups:
The factors that drive behavior are multi-factorial and complex. One health psychology theory divides behavioral factors into three groups:
Capability: Can people open the bottle, administer an injection or use the inhaler? Are they capable of organizing their treatment within their daily lives?
Opportunity: Can people afford the medicines? Do they have easy access to and good communication with their healthcare team? Do they have the support system they need?
Motivation: What beliefs are driving nonadherence? Are they worried about dependency and side effects? Are they depressed and overwhelmed? Do they not believe the medicine will help?
Real World Examples
How does this play out in real life? Your beliefs drive everything you do, each decision you make. You believe a certain director produces only violent or scary films, so you won’t see his newest ones, regardless of reviews to the contrary.
You believe that an occasional cigarette won’t really hurt you, despite warnings from your physician. You believe you only need to apply sunscreen at the beach, ignoring the rising epidemic of skin cancer from daily cumulative UV exposure.
It’s the same situation for health and illness behaviors. Your beliefs may be a more significant factor than clinical data in determining how you manage your illness and/or treatment.
Let’s look at three different patients with asthma — same ages and socio-economic demographics — all prescribed a daily preventer inhaler, which contains steroids, plus an inhaler to use during acute episodes.
Patient No. 1. Bob is fearful of the stigma of “steroids" although the steroids in his daily inhaler carry none of the long-term effects of the steroids he reads about online. He is convinced that his daily inhaler presents more of a danger than benefit, and won’t use it. He will use his other inhaler if he has an attack – but otherwise wants to avoid the medicines altogether.
Patient No. 2 Gary started using his daily inhaler right away, but soon felt he didn’t need it, so he stopped after one week. He doesn’t believe his asthma is “there" all the time because he symptoms come and go, and now he feels fine. Why should he take medication everyday — and pay for that treatment — when the other inhaler helps him during the bad episodes. Seems like a waste of money. Maybe he’ll use it every other day, or a couple of times a week.
Patient No. 3 Dave doesn’t know how to use the inhaler correctly and he’s embarrassed to ask his doctor. His wife will help him if he has an acute attack, he’s survived before so doesn’t think it’s all that important.
If Bob, Gary, and Dave were each to receive reminders to use their daily inhalers, chances are it wouldn’t be successful because they each choose to not take their medicines for different reasons. Likewise, if they were provided with educational support via email, calls, or text, on the importance of taking their daily inhaler, that probably wouldn’t be effective either. Telling someone to do something is rarely effective, especially if you’re telling a person to do something that goes against their beliefs, whether they are guiding a conscious or unconscious decision.
Cost-efficiencies of Personalized Messages
Personalizing a patient support program doesn’t mean someone is handwriting messages to Bob, Gary, and Dave. On the contrary, health psychology frameworks allow us to group people who are motivated by similar beliefs. We can then target people with interventions that precisely address those unhelpful illness perceptions.
Interestingly, the clinical literature shows that even simple text messages can be quite effective in changing beliefs, when applied within a health psychology framework.1 The choice of vehicle only matters in that it needs to resonate with the audience, whether it be texts, phone calls, printed materials web-based or something else.
Once beliefs are changed to drive more healthful behaviors, the results tend to stick for the long-term, making the approach extremely cost-efficient.
Measuring Success
People naturally want to please others, and patients typically want their doctors to think they are following their instructions, even if they’re not. In one study where patient-reported adherence was generally high, the authors found that electronically monitored pill counts and pharmacy-dispensing records correlated more closely with adherence to prescribed quantity than recommended timing of doses2.
Clearly, pill count or pharmacy records, in and of themselves, aren’t a reliable measure for program success, so what is? Just as interventions and support programs need to be personalized to individual beliefs, metrics for success also need to be personalized. For a person being treated for high blood pressure, success can be number of refills (for pharma), regular appointment check-ups (for the HCP) and a clinical response in the form of lower BP numbers (for healthcare systems). But, patients often measure “success" in how they feel. For that reason, level setting and good communication between the HCP and the patient is so important.
What the Future Holds
The application of health psychology to adherence may very well change everything about the way we approach patient care. It allows us to prioritize personalization, and truly places the person at the center of their journey, acknowledging that they’ve been in the driver’s seat all along. The best programs position healthcare stakeholders as guides to the patient, offering clear road maps based on individual circumstances, helping them achieve long-term treatment success.(PV)
Editor’s Notes:
1 Petrie KJ, Perry K, Broadbent E, Weinman J. A text message programme designed to modify patients’ illness and treatment beliefs improves self‐ reported adherence to asthma preventer medication. Br J Health Psychol. 2012;17(1):74-84.
2 Choo, Peter W.; Rand, Cynthia S.; Inui, Thomas S.; Lee, Mei-Ling T.; Cain, Emily; Cordeiro-Breault, Michelle; Canning, Claire; Platt, Richard. In: Medical Care, 9/1/1999, Vol. 37, Issue 9, p. 846-857; J. B. Lippincott Williams and Wilkins Inc. Language: English, Database: JSTOR Journals
Atlantis Healthcare uses health psychology frameworks to design and manage interventions that empower people to better self manage their illness for the long-term.
For more information, visit atlantishealthcare.com.