RNAi therapeutics, a new class of medicines, enable specific and highly effective gene silencing.
RNA interference, also known as RNAi, is a breakthrough in understanding how genes are regulated in cells. RNAi has the potential to change the landscape of medicine and represents a new approach to drug discovery and development.
 Biopharma companies are harnessing the potential of this powerful and complex process to develop treatments for rare diseases as well as common diseases that have a genetic component. By targeting genes that contribute to serious diseases, companies aim to address the underlying cause of illness at the molecular level to restore health.
Biopharma companies are harnessing the potential of this powerful and complex process to develop treatments for rare diseases as well as common diseases that have a genetic component. By targeting genes that contribute to serious diseases, companies aim to address the underlying cause of illness at the molecular level to restore health.
“The RNAi field is just beginning to enter the golden age," says Christopher Anzalone, Ph.D., president and CEO of Arrowhead Pharmaceuticals. “After two decades of intensive study and development, this modality is increasingly being accepted as a reliable and powerful way to treat a variety of diseases."
In 2006, Andrew Fire and Craig Mello, Ph.D., won a Nobel Prize for their discovery of RNA interference and how genes are regulated. That understanding helped to launch a new field of research into potential therapies for genetic and rare diseases.
Now, 14 years later, the company founded by Dr. Mello — Alnylam Pharmaceuticals — has received FDA approval for two RNAi therapies, leading the way in an area of medicine that harnesses a natural process.
Akshay Vaishnaw, M.D., Ph.D., president of R&D at Alnylam Pharmaceuticals, says the advantage of RNAi is that it naturally suppresses genes at the cellular level. The genome is in the nucleus of the cell and contains the blueprints from genes, he says. Those blueprints send out messages to the cytoplasm, the outer part of the cell, where the messages are translated to proteins, which are the building blocks in the body. That process of taking information from the blueprint to the cytoplasm, where the proteins are made, is conducted by an intermediary, the messenger RNA. RNA interference degrades the messenger RNAs specifically based on the sequence of that messenger RNA."
Small interfering RNA (siRNA) are molecules that antagonize the messenger RNAs based on a matching sequence to a specific messenger RNA in a particular disease.
Using RNAi to treat disease presents several important advantages over other approaches to drug development, says Doug Fambrough, Ph.D., president and CEO, Dicerna. Dicerna has created a proprietary technology called GalXC upon which the company develops therapies that silence unhealthy genes.
“RNAi can be used to target any gene because it targets the mRNA that encodes the disease-driving protein," Dr. Fambrough explains. “This allows otherwise ‘undruggable’ targets to be silenced using RNAi."
Dr. Fambrough says RNAi therapies are thought to be a safer option than permanently editing DNA, which could have unknown, unwanted, and irreversible consequences.
 “Conversely, RNAi therapies represent a reversible approach and have the potential for fewer side effects compared with small molecules and antibodies."
“Conversely, RNAi therapies represent a reversible approach and have the potential for fewer side effects compared with small molecules and antibodies."
RNAi therapies also have the potential to reduce the treatment burden on patients. Their long duration of effect means they can be administered through infrequent injections under the skin.
“As the RNAi platform is more broadly applied to drug development, we would expect RNAi-based therapies to become more common in the marketplace in the coming years," Dr. Fambrough says. “We believe RNAi will expand the therapeutic options available to patients, potentially across a spectrum of diseases, including many rare diseases for which there are no currently available treatments."
RNAi Research
In 2018, Alnylam’s Onpattro became the world’s first approved siRNA therapeutic.
Onpattro, which was created to match the messenger RNA for the TTR gene, was approved for the treatment for polyneuropathy of hereditary transthyretin-mediated (hATTR) amyloidosis. This rare disease is caused by a mutation in a gene called transthyretin. The protein misfolds and these misfolded parts are deposited in parts of the body, such as the heart and the nervous system, causing patients to die of heart disease or neuropathy of the nervous system.
“Onpattro reduces the level of the abnormal TTR by 80% or more and as a result patients stabilize or improve from hATTR amyloidosis with peripheral neuropathy," Dr. Vaishnaw says.
The company’s second medicine, Givlaari, was approved in November 2019. Givlaari is for the treatment of adults with acute hepatic porphyria (AHP). AHP is a family of ultra-rare, genetic diseases characterized by debilitating, potentially life-threatening attacks. In acute hepatic porphyria, a gene called ALAS1 in the liver is up-regulated, which results in overproduction of substances that are toxic to nerves. People with the disease are subject to recurring attacks with severe abdominal pain and neuropsychiatric features.
 “Givlaari is an RNAi therapeutic that antagonizes and degrades the ALAS1 message, as a result the toxins that cause these attacks are no longer produced," Dr. Vaishnaw says.
“Givlaari is an RNAi therapeutic that antagonizes and degrades the ALAS1 message, as a result the toxins that cause these attacks are no longer produced," Dr. Vaishnaw says.
Alnylam is advancing a robust pipeline of innovative RNAi-based medicines in four therapeutic areas: genetic diseases, cardio-metabolic diseases, hepatic infectious diseases, and central nervous system and ocular diseases.
Onpattro is in Phase III trials for the cardiac form of hATTR amyloidosis. The company also has a follow-on drug in the hATTR space called vutrisiran, which is in Phase III clinical trials.
Other therapies in Phase III development include fitusiran for hemophilia; lumasiran, a drug for a rare disease called primary hyperoxaluria Type 1; and inclisiran for hypercholesterolemia.
Based on its GalXC technology, Dicerna develops therapies that silence unhealthy genes in a highly targeted, potent, and safe way. The company’s approach is to design proprietary double-stranded RNA molecules that have the potential to engage the enzyme Dicer, the initiation point for RNAi in the human cell cytoplasm, and initiate an RNAi process to silence a specific target gene.
The company’s platform uses a particular Dicer Substrate structure configured for subcutaneous delivery to the liver. Due to the enzymatic nature of RNAi, a single GalXC molecule incorporated into the RNAi machinery can destroy hundreds or thousands of mRNAs from the targeted gene.
Dicerna’s most advanced program is DCR-PHXC, which is in Phase II/III pivotal development for the treatment of patients with all three genetic forms of primary hyperoxaluria (PH). PH is a family of severe, rare, genetic liver disorders characterized by overproduction of oxalate, a natural chemical in the body that is normally eliminated as waste through the kidneys. In patients with PH, the kidneys are unable to eliminate the large amount of oxalate that is produced, and the accumulation of oxalate can result in severe damage to the kidneys and other organs. Currently, there are no approved therapies for the treatment of PH.
The company has several other programs in its pipeline, including DCR-HBVS, which is in a Phase I clinical trial for the treatment of patients with chronic hepatitis B virus (HBV) infection, in partnership with Roche; DCR-A1AT, which is in a Phase I/II clinical trial for the treatment of patients with alpha-1 antitrypsin deficiency-associated liver disease; and a preclinical program for an undisclosed indication.
 "RNAi has become an increasingly attractive area of research, with multiple companies pursuing RNAi technology and exploring its use in new therapeutic areas," Dr. Fambrough says. “Our GalXC technology represents a differentiated approach to RNAi."
"RNAi has become an increasingly attractive area of research, with multiple companies pursuing RNAi technology and exploring its use in new therapeutic areas," Dr. Fambrough says. “Our GalXC technology represents a differentiated approach to RNAi."
He says data from clinical and preclinical studies suggest that GalXC may offer several distinct benefits for the treatment of disease, including increased potency, specific binding to disease-causing targets, long duration of action, and a subcutaneous dosing regimen.
Another company developing RNAi therapies is Arrowhead Pharmaceuticals. The company has a proprietary targeted RNAi molecule (TRiM) platform.
Arrowhead has a broad pipeline of RNAi therapies to treat intractable diseases, including liver disease, cardiovascular disease, cystic fibrosis, and cancer.
The company’s most advanced candidate, ARO-AAT, is being developed for the treatment of liver disease associated with alpha-1 antitrypsin deficiency. Arrowhead is currently conducting an ongoing, potentially pivotal Phase II/III trial.
Arrowhead is also developing cardiovascular candidates that address well-validated cardiometabolic targets. ARO-APOC3 is currently in Phase I to reduce levels of apoC-III for the treatment of severe hypertriglyceridemias, initially addressing familial chylomicronemia syndrome (FCS). ARO-ANG3 is currently in Phase I to reduce plasma lipoprotein levels for the treatment of various types of dyslipidemias. The company expects to initiate Phase III clinical trials for both drug candidates in 2020.
Arrowhead has a partnership with Janssen for JNJ-3989, which is currently in a REEF-1 Phase IIb combination study for the treatment of chronic hepatitis B. Arrowhead is also partnering with Amgen on AMG-890, which is currently in Phase I study for the treatment of cardiovascular disease.
Challenges of Developing RNAi Therapeutics
The possibilities for RNAi are as great as the challenges, one of the biggest challenges being that the delivery of the drug has to pass the blood-brain barrier, particularly for CNS diseases.
Another challenge manufacturers have in developing siRNAs is that they are short-lived, says Daniel Kavanagh, Ph.D., senior scientific advisor, gene therapy, WCG.
“This is being addressed by changing the natural chemistry of the ribonucleic acids by a variety of methods, in essence these are chemically-modified RNAs," he says. “The other big challenge is delivery to the right part of the right cells. Some companies are using nanoparticles and attaching specific sugars to the outside to try to get them to the right cells. In terms of target organs, the liver is a relatively easy organ to get to, which helps explain why the first approved RNAi drugs target the liver."
Traditional gene therapy is a good approach to address autosomal recessive diseases, he says, because recessive mutant genes usually don’t play any functional role in cells, which means the function can be restored by simple gene replacement.
 “But for autosomal dominant diseases, including the indications for the first approved siRNA treatments, it’s not good enough to introduce a functional form of the gene," Dr. Kavanagh says. “siRNA is a knockdown strategy and will likely be a primary approach of choice, in addition to CRISPR gene editing, for autosomal dominant diseases. Although the first FDA-approved RNAi products are not allele-selective, RNAi is sufficiently specific and targetable that it’s possible to selectively knock down the mutant allele. This no doubt will be a likely focus of the next generation of siRNA products."
“But for autosomal dominant diseases, including the indications for the first approved siRNA treatments, it’s not good enough to introduce a functional form of the gene," Dr. Kavanagh says. “siRNA is a knockdown strategy and will likely be a primary approach of choice, in addition to CRISPR gene editing, for autosomal dominant diseases. Although the first FDA-approved RNAi products are not allele-selective, RNAi is sufficiently specific and targetable that it’s possible to selectively knock down the mutant allele. This no doubt will be a likely focus of the next generation of siRNA products."
Alnylam encapsulated its RNAi therapeutic in a lipid nanoparticle (LNP), which allows it to be delivered to the hepatocyte. “We did an enormous amount of research to demonstrate the mechanism of action and to design LNPs appropriately," Dr. Vaishnaw says. This is the process that drove the Onpattro program.
For Givlaari, the company developed another delivery mechanism, a GalNAc conjugate, which provides advantages over the LNP process.
"We attached a sugar N-acetyl galactosamine, and the hepatocyte recognizes that sugar and the drug goes to the liver via the blood. The receptor on the hepatocyte grabs that sugar and takes the siRNA into the liver cell."
Dr. Vaishnaw says all of the therapies in Alnylam’s pipeline with the exception of Onpattro use the GalNAc conjugate. “While the Onpattro is given once every three weeks, some therapies with GalNAc conjugates only need to be given to patients once every three months or once every six months," he says.
Commercializing New RNAi Therapies
While several gene therapies have been approved, it is an emerging area of medicine.
Therefore it is of critical importance to educate all stakeholders, from physicians to patients and the general public, on what RNA/RNAi is and the differences among new gene therapies and gene editing technologies.
There is a lot of misunderstanding and a lack of knowledge among physicians. In fact, there is significant confusion among prescribers regarding several aspects of nucleic acid-based therapies, according to a survey by InCrowd. Only 56% of screened respondents reported being somewhat familiar with RNA- or DNA-based therapeutic methods. “I was surprised by the amount of misinformation, lack of understanding, and lack of knowledge in this space," says Diane Hayes, Ph.D., co-founder of InCrowd. “Even when physicians said they were pretty familiar with different therapeutic areas in the space, they were unable to name the drugs that were on the market."
Only 7% of respondents in InCrowd’s survey report high familiarity with gene therapy. Not surprisingly, Dr. Hayes says, oncologists had the highest familiarity of the specialists surveyed.
“Oncology is an ever-changing field," Dr. Hayes says. "Oncologists are keen on staying current with changes in the field.
Dr. Hayes says when marketing gene therapies to physicians, it’s important to go back to basics, and make sure physicians understand how gene therapies work and how they differ from previous approaches.
Another challenge is the unprecedented costs associated with these therapies. The current system of health insurance that is based on unit pricing is not set up to address high-cost, and sometimes one-time, cell and gene therapies.
"The cost of healthcare is an important discussion in our society and encompasses more than drug pricing," Dr. Fambrough says. “Our goal is to provide innovative and life-changing therapies to people living with rare genetic diseases and common diseases that have a genetic component by addressing the underlying cause of illness. We are focused on understanding the unique disease-related burdens of patients and their caregivers as we create new  medicines with the potential to restore their health and better serve and support the wider patient community. By forming strong, two-way connections with patient communities, we can learn from each other and uncover important insights that guide the development of compelling new medicines and support services."
medicines with the potential to restore their health and better serve and support the wider patient community. By forming strong, two-way connections with patient communities, we can learn from each other and uncover important insights that guide the development of compelling new medicines and support services."
Biopharmaceutical companies, payers, and providers are working together to find a new structure that allows patients to realize the benefits of these new therapies. They are forming unique reimbursement and contracting structures that aim to address the needs of patients, while making it financially feasible for payers. A common theme among these arrangements is outcomes- and value-based contracting.
When Alnylam announced Onpattro’s approval in 2018, it also announced that it had arranged value-based agreements with leading health insurers. So far, the company has agreements with Harvard Pilgrim Health Care and other major health insurers, and is engaging in other ongoing discussions.
Based on MMIT, a leading medical policy-reporting agency, the contracts with these payers cover about 76% of commercial medical lives in the United States. The agreements are structured to link Onpattro’s performance in real-world use to financial terms.
Providers will assess Onpattro patients in terms of their overall symptomology, for example their ability to walk or their autonomic dysfunction. If patients are not getting better, Alnylam will provide a discount. The company also is working with CMS to provide access to those covered by Medicare.
The company currently has 10 value-based agreements assigned, and those along with government agreements, cover 98% of U.S. lives.
Alnylam also launched Alnylam Assist, a comprehensive support services program to help patients. Alnylam Assist offers a wide range of personalized services that include access to in-house case managers who help with verification of insurance benefits and financial support for eligible patients, and field-based patient education liaisons who offer patient education on hATTR amyloidosis.
For Givlaari, Alnylam implemented several steps to keep costs under control, including value-based agreements with payers that provide rebates for patients who don’t respond. The company is working with health insurers such as Cigna Corp. and state Medicaid agencies. The company will also help patients verify their insurance benefits and help with financial assistance.
Dr. Vaishnaw says these value-based agreements and the prevalence-based adjustment features are sound ways for a company like Alnylam that’s engaged in innovation to be rewarded and be a responsible party.(PV)
~~~~~~~~~~~~~~~~~~~~~~~~~
Physician Awareness of Gene Therapies
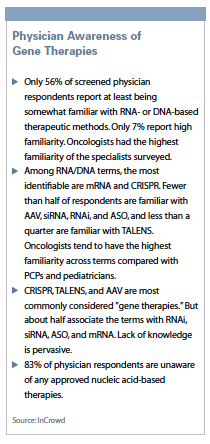
Only 56% of screened physician respondents report at least being somewhat familiar with RNA- or DNA-based therapeutic methods. Only 7% report high familiarity. Oncologists had the highest familiarity of the specialists surveyed.
Among RNA/DNA terms, the most identifiable are mRNA and CRISPR. Fewer than half of respondents are familiar with AAV, siRNA, RNAi, and ASO, and less than a quarter are familiar with TALENS. Oncologists tend to have the highest familiarity across terms compared with PCPs and pediatricians.
CRISPR, TALENS, and AAV are most commonly considered "gene therapies." But about half associate the terms with RNAi, siRNA, ASO, and mRNA. Lack of knowledge is pervasive.
83% of physician respondents are unaware of any approved nucleic acid-based therapies.
Source: InCrowd